Association of Oral Contraceptives Consumption with C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin (IL-6) in Female in vivo Model
-
Barizoge Cletus Lemii
Department of Pharmacology and Therapeutics, Faculty of Basic Clinical Sciences, College of Medical Sciences, Port Harcourt, Rivers State University, Nigeria
Iyaeneomi Ransome DakaDepartment of Pharmacology and Therapeutics, Faculty of Basic Clinical Sciences, College of Medical Sciences, Port Harcourt, Rivers State University, Nigeria
Christine Umanu Gabriel-BrisibeDepartment of Medical Biochemistry, Faculty of Basic Medical Sciences, College of Medical Sciences, Rivers State University, Nigeria
Sarah Kelechi EnebeliDepartment of Pharmacology and Therapeutics, Faculty of Basic Clinical Sciences, College of Medical Sciences, Port Harcourt, Rivers State University, Nigeria
Ucheawaji Felicia EdwardDepartment of Pharmacology and Therapeutics, Faculty of Basic Clinical Sciences, College of Medical Sciences, Port Harcourt, Rivers State University, Nigeria
Iyingiala Austin-AsomejiDepartment of Community Medicine, Faculty of Clinical Sciences, College of Medical Sciences, Rivers State University, Nigeria
Efekemo OghenetekevweDepartment of Chemical Sciences, Biochemistry Programme, Faculty of Science, Edwin Clark University, Kiagbodo, Delta, Nigeria
Nodi Conquest ChivusalemDepartment of Biochemistry, Faculty of Science, Port Harcourt, Rivers State University, Nigeria
Tamuno-Boma Odinga-Israel

Department of Biochemistry, Faculty of Science, Port Harcourt, Rivers State University, Nigeria
| Received 09 Jun, 2024 |
Accepted 11 Jul, 2024 |
Published 12 Jul, 2024 |
Background and Objective: Inflammatory biomarkers like C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin-6 (IL-6) are implicated in lots of inflammatory and auto-immune disorders and thus often used as tools for prediction of disease risk. The study aimed to determine the effects of oral contraceptive pills (Exluton and Combi-3) on these inflammatory biomarkers. Materials and Methods: The 25 adult female albino Wistar rats were obtained from the Animal House of Rivers State University, Port Harcourt and were divided into 5 groups of 5 Wistar rats each-Control, 200, 400 mg/kg Exluton, 200 and 400 mg/kg Combi-3 groups. They were allowed standard feed and water ad libitum to acclimatize for 14 days, after which the test drugs were administered to the various groups for 21 days. The rats were sacrificed and blood samples were collected for assessment of CRP, TNF and IL-6 using standard laboratory procedures. Data obtained were subjected to IBM SPSS, version 25 for statistical analysis. Results: The results for CRP revealed a non-significant (p>0.05) decrease in the groups 200, 400 mg/kg Exluton and 200 mg/kg Combi-3 and a nonsignificant (p>0.05) elevation of 400 mg/kg Combi-3 group. The result for IL-6 demonstrated a significant (p<0.05) elevation and reduction in 200 and 400 mg/kg Exluton groups, respectively and a non-significant (p>0.05) increase and decrease in 200 and 400 mg/kg Combi-3, respectively. The findings for TNF showed that a significant elevation was observed in TNF on administration of Exluton and Combi-3 when all were compared with the control groups. Conclusion: The oral contraceptives of study tend to inhibit elevation of C-reactive protein and have variable changes on IL-6, tending to decrease it at high doses. A markedly significant increase in TNF was also observed. This increase in TNF could account for the potential risk in incidences of autoimmune, cardiovascular, neurodegenerative and other metabolic risks associated with oral contraceptives.
| Copyright © 2024 Lemii et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Inflammatory processes play an underlying role in disease/cancer pathogenesis. For example, in hypertension, which is a prominent cardiovascular disease there is an increase in the level of pro-inflammatory cytokines in the blood and tissues of the cardiovascular system1. Several inflammatory biomarkers in the blood have been assessed as potential tools for predicting the risk of certain diseases2. Biomarkers of systemic inflammation, such as C-Reactive Protein (CRP), serum amyloid A, cytokines like Interleukin-6 (IL-6) and Monocyte Chemotactic Protein-1 (MCP-1), as well as adhesion molecules including Soluble Intercellular Adhesion Molecule type 1 (sICAM-1) and Tumor Necrosis Factor (TNF), have been evaluated as potential tools for predicting disease risk.
The C-Reactive Protein (CRP), a biomarker of acute inflammation, is an acute-phase protein produced by liver cells in response to pro-inflammatory cytokines during inflammatory/infectious processes and determines the risk of chronic neurodegenerative diseases like cardiovascular diseases, diabetes mellitus, Alzhemers’s and Parkinson’s diseases3.
The circulating level of CRP is commonly used as an inflammatory marker to assess the risk for Cardiovascular Disease (CVD) and stroke4. Published studies attested correlations between pro-inflammatory cytokines relating the CRP levels and the severity of the atherosclerotic process5. Previous and recent human population-based studies6-10 reported positive correlation between CRP rise and intake of oral contraceptive use.
Interleukins are any of a set of naturally occurring proteins that mediate and control cell communication, cell growth, differentiation and motility. They are especially critical for triggering immunological responses11.
Interleukin 6 (IL-6) is a mediatory endogenous molecule that acts as a pro-inflammatory cytokine12. The IL-6 stimulates the inflammatory and auto-immune processes in many diseases such as multiple sclerosis, Neuromyelitis Optica Spectrum Disorder (NMOSD), diabetes, atherosclerosis/thromboembolism, depression, Alzheimer's disease, systemic lupus erythematosus, multiple myeloma, prostate cancer, Behçet’s disease, rheumatoid arthritis and intracerebral hemorrhage13. The IL-6 is increased in normal menstruating females than in females on oral contraceptive pills according to reports14,15 which depicts a reduction in the concentration of IL-6. However, Ayub et al.16 noted elevated serum levels of IL-6 in users of oral contraceptive pills. In their studies, Sim et al.17 and Manzoor et al.18 observed no difference in the serum concentration of IL-6 in females taking or not on doses of oral contraceptives. Recently, there has been increasing interest in developing anti-IL-6 agents as therapy against many non-communicable diseases19.
Tumor Necrosis Factor-α (TNF-α) is a cytokine-a protein, molecule and hormone-like substance that plays a crucial role in many cellular processes, including growth, differentiation, migration and apoptosis20. Variations in the serum concentration of the cytokine Tumor Necrosis Factor-α (TNF-α) may have potential as a biomarker for Multiple Sclerosis (MS), which is an inflammatory and neurodegenerative disease21. For patients with rheumatoid arthritis who were treated aggressively, they had low levels of the cytokine Tumor Necrosis Factor (TNF) in their serum, which confirmed the important role of TNF in the inflammatory process associated with rheumatoid arthritis22. Cardiovascular diseases and cancers are considered pro-inflammatory conditions, characterized by increased secretion or levels of inflammatory biomarkers such as the cytokine Tumor Necrosis Factor Alpha (TNF-α)23-25. The cytokine Tumor Necrosis Factor (TNF) is involved in all stages of carcinogenesis, including cellular transformation, proliferation, angiogenesis (blood vessel formation) and metastasis26. The TNF-α is one of the most important cytokines responsible for the endothelial dysfunction that is characteristic of hypertension27,28. The TNF has also been implicated in the pathogenesis of several disease states, including rheumatoid arthritis, ankylosing spondylitis and Crohn's disease29.
Other studies have provided consistent evidence that the risks of breast and cervical cancers are increased, whereas the risks of endometrial, ovarian and colorectal cancers are reduced in women who use oral contraceptives30,31. Oral contraceptive use was associated with increased fold expression of inflammatory markers including TNF with attendant metabolic abnormalities32.
One recent hormonal contraceptive is lynestrenol, commercially marketed as Exluton. Exluton is a progestogen-only oral contraceptive pill that contains the progestogen lynestrenol (ATC class G03AC02). Like other progestogen-only pills, lynestrenol is well-suited for use during breastfeeding and for women who may not want or are unable to use estrogens. Within the body, lynestrenol is metabolized into the biologically active metabolite norethisterone, which then binds to the progesterone receptors in target organs such as the uterine muscle (myometrium)7. The contraceptive mechanism of action of lynestrenol (the active ingredient in the contraceptive pill Exluton) is achieved primarily by increasing the viscosity and thickness of the cervical mucus, which in turn reduces the ability of sperm to penetrate and reach the egg5.
Combination 3 is a combination of synthetic estrogen and progestin-containing oral contraceptives hormonal pills that prevent the ovaries from producing an egg. They also alter cervical mucus and the uterine lining (endometrium) milieu to prevent sperm from attaching to the egg33. Combination 3 is also used in the treatment of polycystic ovarian syndrome (POS)34.
Exulton and combination 3 are oral contraceptives used by women of both reproductive and non-childbearing categories but could have potential to initiate processes leading to some non-communicable diseases or medical conditions via their effects on pro-inflammatory biomarkers. Thus, considering the positive correlation between bio-inflammatory markers (TNF, CRP and IL) and regularly consumed contraceptive pills in previous studies, it is imperative to choose Exulton and combination 3 being commonly used and most times abused and having a paucity of data. Also, most available studies that reported on effects of contraceptive pills on these biomarkers are done at a retrospective level. Thus, there is a need to describe the correlation between selected oral contraceptives in this study and the commonly implicated inflammatory biomarkers (C-reactive protein, interleukin 6 and TNF) using an experimental approach. This study explored the effects of oral contraceptive pills (Exluton and Combi-3) on the inflammatory biomarkers: C-reactive protein, interleukin 6 and TNF.
MATERIALS AND METHODS
Study duration: This study was carried out from September, 2021 to February, 2022.
Experimental animals: The 25 adult female albino rats were obtained from the animal house of Rivers State University, Port Harcourt and taken to the experimental laboratory where they were divided into 5 groups of 5 albino rats each. They were given standard feed and water ad libitum and allowed to acclimatize for 14 days.
Drug of study: Exluton is a brand of progesterone-only pill containing specifically 500 μg of lynestenol in each tablet. Combination 3 pills is a Combined Oral Contraceptive Pill (COCP) containing levonorgestrel 0.15 mg and ethinyl estradiol 0.03 mg and an iron-based compound, iron fumarate. The combination 3 pack consists of 21 white hormonal tablets and 7 non-hormonal tablets. Each white hormonal tablet contains low doses of estrogen and progesterone hormones. Both drugs were purchased from a Medical Pharmacy in Port Harcourt, Rivers State, Nigeria.
Experimental grouping/drug administration, Odinga et al.35:
The female albino rats were divided into 5 groups:
| Group 1 | : | Feed+water only | |
| Group 2 | : | 200 mg/kg Exluton+feed+water (low dose-LD Exluton) | |
| Group 3 | : | 400 mg/kg Exluton+feed+water (high dose-HD Exluton) | |
| Group 4 | : | 200 mg/kg Combination 3+feed+water (low dose-LD Combi-3) | |
| Group 5 | : | 400 mg/kg Combination 3+feed+water (high dose-HD Combi-3) |
Administration of drugs was as reported by Odinga et al.36. Each day a tablet is dissolved in 100 mL distilled water and the appropriate dose per kg was measured out using a 2 mL syringe for oral administration via an oro-gastric tube. Low dose received 0.14 mL while the high dose received 0.30 mL of the prepared drug. These doses were determined based on comparative dosage per body weight proportion akin to humans.
Sample collection and procedure: On the last day (21st day from onset of medication), the rats were fasted overnight, weighed and euthanized and were sacrificed by placing them in a desiccator. Blood samples were collected and stored in a plain sample bottle. The blood was centrifuged at 3000 rotations per minute for 3 min and the blood plasma was separated and used for the analysis.
Sample analysis: Normal rat plasma (NRP) was prepared from rat blood collected in the anticoagulant EDTA (10 mM). The blood was centrifuged for 10 min at 1300 g to separate the plasma supernatant. This plasma supernatant was then supplemented with calcium chloride (CaCl2) to a final concentration of 12 mM. After incubating this recalcified plasma for 20 min at 37°C, the resulting fibrin clot was removed by centrifugation at 1300 g for 15 min at 4°C. Finally, the recalcified normal rat plasma was aliquoted and stored at -70°C until needed for activation experiments. A similar procedure was used to obtain recalcified normal human plasma (NHP).
Purified rabbit antibodies against C-RP (1 μg/mL) were used as catching antibodies. The samples to be tested were serially diluted in PBS containing 0.1% (wt/vol) Tween 20 and 0.2% (w/v) gelatin (PTG). Biotinylated anti-C-RP was diluted in ELISA-ultra performance buffer supplemented with 10 mm EDTA. Plates were developed with strept-PO. Purified C-RP was used as a standard. Hundred millilitre (100 mL) of standard sample were added to each well and incubated for 2 hrs at 37°C. As 100 μL biotin-antibody (1×) were added to each well and incubated for 1 hr at 37°C then aspirated and washed 3 times. Another 100 μL HRP-avidin (1×) was added to each well and incubated for 1 hr at 37°C and the aspirate was washed 5 times before adding 90 μL TMB substrate to each well. It was incubated for 15-30 min at 37°C and protected from light, then added 50 μL of stop solution to each well and read at 450 nm within 5 min.
Serum was prepared for TNF-α determinations and were stored at -70°C until they were analyzed. The TNF-α was measured by commercial ELISA (R&D) Systems, according to the manufacturer's instructions.
Statistical analysis: Data were analyzed using SPSS (statistical package for social sciences) version 25.0. Statistical evaluations of the difference between the group mean values were tested by One-way Analysis of Variance (ANOVA) and tukey’s post hoc test for multiple comparisons. The results were expressed as Mean±Standard deviation and statistical significance was considered at p<0.05.
RESULTS
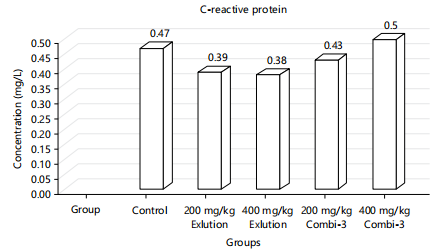
In Table 1 and Fig. 1, C-reactive protein values for groups-LD Exluton, HD Exluton and LD Combi are lower insignificantly (p<0.05) in comparison with the control group in the decreasing order as follows: LD Combi>LD Exluton>HD Exluton. The group 5 administered with HD Combi-3 increased insignificantly (p>0.05) when compared to the control. Thus, CRP decreases insignificantly (p>0.05) with increasing doses of Exluton (HD and LD) and LD Combi-3 but increases insignificantly (p>0.05) with increasing doses of HD Combi-3 when compared with the control.
|
|
| Table 1: | Effect of exluton and combination 3 on the C-reactive protein, tumor necrosis factor and interleukin-6 biomarkers | |||
| Parameter | Control | 200 mg/kg Exluton | 400 mg/kg Exluton | 200 mg/kg Combi-3 | 400 mg/kg Combi-3 |
| CRP (mg/mL) | 0.47±0.12a | 0.39±0.03a | 0.38±0.06a | 0.43±0.08a | 0.50±0.05a |
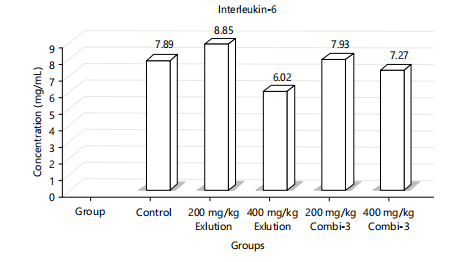
| IL-6 (pg/mL) | 7.89±0.55a | 8.85±1.35a,c | 6.02±0.49a,b | 7.93±1.02a | 7.27±1.41a |
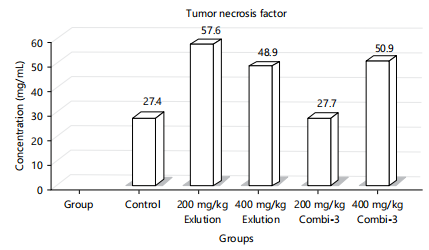
| TNF (pg/mL) | 27.400±8.745a | 57.575±7.008b | 48.900±29.405c | 27.680±11.253a | 50.925±12.089d |
| Values are expressed as Mean±Standard Deviation, Values with the same superscript on the same row show no significant difference at (p<0.05), Values with different superscript in the same row shows significant difference at (p<0.05), CRP: C-reactive protein, TNF: Tumor necrosis factor and IL-6: Interleukin-6 | |||||
In Table 1 and Fig. 2, Interleukin-6 (IL-6) values for the groups administered with combination 3, HD combi at key value of (7.27±2.08) was insignificantly (p>0.05) lower when compared to the control (7.89±0.55), LD Combi (7.93±1.02) was insignificantly (p>0.05) higher compared to the control (7.89±0.55).
|
For interleukin-6 value in the groups administered with Exluton, there was a significant (p<0.05) increase in LD Exluton value at (8.85±1.35) compared with the control group (7.89±0.55). The HD Exluton at (6.02±0.49) was lower significantly (p<0.05) in value when compared to the control (7.89±0.55). Thus, the values of IL-6 decrease significantly (p<0.05) with increasing doses of Exluton and with an insignificant (p>0.05) decrease with increasing doses of Combi 3.
From Table 1 and Fig. 3, the values of TNF when compared with the control group showed that both LD exluton and HD exluton administered groups had a significant (p<0.05) elevation in TNF. The groups administered with combination-3, revealed a significant (p<0.05) increase in LD Combi-3 and a non-significant (p<0.05) increase in TNF when compared with the control group, respectively.
DISCUSSION
According to Table 1 and Fig. 1, C-reactive protein values for groups-LD Exluton, HD Exluton and LD Combi are lower insignificantly (p<0.05) in comparison with the control group in the decreasing order as follows: LD Combi>LD Exluton>HD Exluton. Thus, CRP decreases insignificantly (p<0.05) with increasing doses of Exluton (HD and LD) and LD Combi-3 but increases insignificantly (p<0.05) with increasing doses of HD Combi-3 when compared with the control.
These findings agreed with the findings from previous studies37-42 which reported a significant increase in CRP in women on combined contraceptive use thus predisposing them to risk of cardiovascular diseases. The insignificant decrease in the group treated with Exluton which is a progesterone-only contraceptive might be attributable to the absence of estrogen. Various risks associated with increased serum concentration of CRP including cardiovascular, arteriosclerotic and neurodegenerative risks were reported by Banait et al.43 and therefore chronic intake of combination-3 could predispose women to such risks while Exluton contraceptive, containing progesterone only could reduce such risk.
In Table 1 and Fig. 2, the values of IL-6 decrease significantly (p<0.05) with increasing doses of Exluton and with an insignificant (p<0.05) decrease with increasing doses of Combi 3.
These findings to some extent differ from the findings of Larsen et al.44 which showed that there is no difference in concentration of IL-6 in females on or not on oral contraceptives. However, IL-6 was found to increase in normal menstruating females than in females on oral contraceptive pills according to reports as well as studies which depict a reduction in the concentration of IL-645. This asserts some position in this research which demonstrated a significant reduction in the levels of groups treated with HD Exluton and a non-significant reduction of those treated with HD combi 3. However, elevated serum levels of IL-6 in users of oral contraceptive pills which established the same result seen in treatment groups LD Exluton and LD Combi-3 with significant and non-significant elevated concentration levels respectively were also reported by Sim et al.17 and Eagan et al.45. The IL-6 stimulates the inflammatory and auto-immune processes in many diseases and thus women on LD Exluton and LD Combi-3 can predispose such candidates to these diseases. Also, there is increasing interest in developing anti-IL-6 agents as therapy against many non-communicable diseases46 and by implication, doses of HD Exluton could be explored for this remedy.
From Table 1 and Fig. 3, the values of TNF when compared with the control group showed that both LD exluton and HD exluton administered groups had a significant (p<0.05) elevation in TNF and therefore validated studies by Divani et al.42 and Yousuf et al.34 which indicated that oral contraceptive pill treatment of 6 months duration of women with polycystic ovarian syndrome increases plasma ICAM-1, MCP-1 and TNF-α levels and these cytokines also correlate positively with many metabolic parameters including plasma glucose, lipids and homeostatic model assessment-insulin resistance. The groups administered with combination-3, revealed a significant (p<0.05) increase in LD Combi-3 and a non-significant (p<0.05) increase in TNF when compared with the control group, respectively. This again establishes the same position in previous studies stated above. Increased TNF is implicated in lots of metabolic, neurodegenerative diseases and other non-communicable diseases as reported by experimental findings in previous studies47.
The findings of this study suggest the possible and attributable cardiovascular risks like thromboembolism and cervical and breast cancer with the use of oral contraceptives, most especially when abused, which is common in most tertiary institution campuses. These effects are most likely in females. Although, this study is not the first to investigate the use of oral contraceptives, the study explored its effects specifically on the effect of commonly abused oral contraceptives and its effects on the inflammation markers. It is therefore recommended that the use of oral contraceptives should be in strict adherence to the prescribed doses and time. The researchers recommend an investigation into the use of oral contraceptives on other inflammation markers that were not included in this study. Also, an investigation into some metabolic condition markers that predispose to cardiovascular risk and malignancy is recommended.
CONCLUSION
This study suggests that oral contraceptives especially the progesterone component caused a decrease in CRP serum levels and thus could inhibit inflammatory responses in body cells with attendant reduction in the risk of cardiovascular and neurodegenerative diseases. A variable change in IL-6 in this study with overriding tendencies of decreased serum concentration at chronic or high doses could result in decreased incidences of auto-immune processes involving multiple sclerosis, diabetes atherosclerosis and multiple myeloma among others individuals on oral contraceptives. However, an increase in TNF tends to counter this correlation and is most likely responsible for the attributable cardiovascular risk like thromboembolism and cervical and breast cancer assosiated with the use of oral contraceptive use.
SIGNIFICANCE STATEMENT
Oral contraceptives have been effectively used by women. However, it could have the potential to initiate processes leading to non-communicable diseases or medical conditions via its effects on pro-inflammatory biomarkers. Considering that most available studies that reported on the effects of contraceptive pills on these biomarkers are done at a retrospective level, there is a need to describe the correlation between selected oral contraceptives in this study and the commonly implicated inflammatory biomarkers using an experimental approach. This study suggests that oral contraceptives might inhibit the elevation of CRP and cause variable changes in IL-6, tending to decrease it at high doses and a significantly increased TNF. This increase in TNF could account for the potential risk in incidences of autoimmune, cardiovascular, neurodegenerative and other metabolic risks associated with oral contraceptives.
ACKNOWLEDGMENTS
The authors express their gratitude to Mr. Barine and Students of Biochemistry, Faculty of Science (Rita Olofu and the Exluton team) for their assistance in carrying out the bench work and technical support.
REFERENCES
- Libby, P., 2017. Interleukin-1 beta as a target for atherosclerosis therapy: Biological basis of CANTOS and beyond. J. Am. Coll. Cardiol., 70: 2278-2289.
- Obeng-Aboagye, E., A. Frimpong, J.A. Amponsah, S.E. Danso, E.D.A. Owusu and M.F. Ofori, 2023. Inflammatory cytokines as potential biomarkers for early diagnosis of severe malaria in children in Ghana. Malar. J., 22.
- Ding, Z., Y. Wei, J. Peng, S. Wang, G. Chen and J. Sun, 2023. The potential role of C-reactive protein in metabolic-dysfunction-associated fatty liver disease and aging. Biomedicines, 11.
- Choi, J., L. Joseph and L. Pilote, 2013. Obesity and C-reactive protein in various populations: A systematic review and meta-analysis. Obesity Rev., 14: 232-244.
- Stewart, J.C., K.L. Rand, M.F. Muldoon and T.W. Kamarck, 2009. A prospective evaluation of the directionality of the depression-inflammation relationship. Brain Behav. Immun., 23: 936-944.
- van Rooijen, M., L.O. Hansson, J. Frostegård, A. Silveira, A. Hamsten and K. Bremme, 2006. Treatment with combined oral contraceptives induces a rise in serum C-reactive protein in the absence of a general inflammatory response. J. Thromb. Haemostasis, 4: 77-82.
- Kelly, E., C.A. Owen, V. Pinto-Plata and B.R. Celli, 2013. The role of systemic inflammatory biomarkers to predict mortality in chronic obstructive pulmonary disease. Expert Rev. Respir. Med., 7: 57-64.
- Lopa, S.S., F. Hasan, A.M. Jamil, S.A. Lima, M. Islam and R. Haque, 2022. Effect of hormonal contraceptives on inflammatory blood biomarker C-reactive protein. Int. J. Pharm. Sci. Res., 13: 2689-2696.
- Mouliou, D.S., 2023. C-reactive protein: Pathophysiology, diagnosis, false test results and a novel diagnostic algorithm for clinicians. Diseases, 11. https://doi.org/10.3390/diseases11040132
- Badenhorst, C.E., A.D. Govus and T. Mündel, 2023. Does chronic oral contraceptive use detrimentally affect C-reactive protein or iron status for endurance-trained women? Physiol. Rep., 11.
- Borish, L.C. and J.W. Steinke, 2003. 2. Cytokines and chemokines. J. Allergy Clin. Immunol., 111: S460-S475.
- Kong, B.S., Y. Kim, G.Y. Kim, J.W. Hyun, S.H. Kim, A. Jeong and H.J. Kim, 2017. Increased frequency of IL-6-producing non-classical monocytes in neuromyelitis optica spectrum disorder. J. Neuroinflammation, 14.
- Kristiansen, O.P. and T. Mandrup-Poulsen, 2005. Interleukin-6 and diabetes: The good, the bad, or the indifferent? Diabetes, 54: S114-S124.
- Mascone, S.E., D.W. Jacob, L.E. Eagan, J.L. Harper, J.K. Limberg and S.M. Ranadive, 2023. Naturally menstruating women exhibit lower cardiovagal baroreflex sensitivity than oral contraceptive users during the lower hormone phase. Exp. Physiol., 108: 1481-1489.
- Kamp, K.J., C. Han, R.J. Shulman, K.C. Cain and P. Barney et al., 2021. Cytokine levels and symptoms among women with irritable bowel syndrome: Considering the role of hormonal contraceptive use. Biol. Res. Nurs., 23: 171-179.
- Ayub, H., N. Saba, L. Malik, Z. Rauf, T. Fatima and K. Rehman, 2021. Serum interleukin-6, C-reactive protein and enzymatic profile variations as potential biomarkers of hormonal oral contraceptive induce damages. Arch. Obstet. Gynecol. Reprod. Med., 4: 104-112.
- Sim, M., B. Dawson, G. Landers, D.W. Swinkels and E. Wiegerinck et al., 2017. Interleukin-6 and hepcidin levels during hormone-deplete and hormone-replete phases of an oral contraceptive cycle: A pilot study. Ann. Nutr. Metab., 70: 100-105.
- Manzoor, S., M.A. Ganie, S. Amin, Z.A. Shah and I.A. Bhat et al., 2019. Oral contraceptive use increases risk of inflammatory and coagulatory disorders in women with polycystic ovarian syndrome: An observational study. Scient. Rep., 9..
- Dowlati, Y., N. Herrmann, W. Swardfager, H. Liu, L. Sham, E.K. Reim and K.L. Lanctôt, 2010. A meta-analysis of cytokines in major depression. Biol. Psychiatry, 67: 446-457.
- Laha, D., R. Grant, P. Mishra and N. Nilubol, 2021. The role of tumor necrosis factor in manipulating the immunological response of tumor microenvironment. Front. Immunol., 12.
- Paul, A., M. Comabella and R. Gandhi, 2018. Biomarkers in multiple sclerosis. Cold Spring Harbor Perspect. Med., 9.
- Mateen, S., S. Moin, S. Shahzad and A.Q. Khan, 2017. Level of inflammatory cytokines in rheumatoid arthritis patients: Correlation with 25-hydroxy vitamin D and reactive oxygen species. PLoS ONE, 12.
- Zhang, H. and N.S. Dhalla, 2024. The role of pro-inflammatory cytokines in the pathogenesis of cardiovascular disease. Int. J. Mol. Sci., 25.
- Alfaddagh, A., S.S. Martin, T.M. Leucker, E.D. Michos and M.J. Blaha et al., 2020. Inflammation and cardiovascular disease: From mechanisms to therapeutics. Am. J. Preventive Cardiol., 4.
- Bikomeye, J.C., A.M. Beyer, J.L. Kwarteng and K.M.M. Beyer, 2022. Greenspace, inflammation, cardiovascular health, and cancer: A review and conceptual framework for greenspace in cardio-oncology research. Int. J. Environ. Res. Public Health, 19.
- Wang, X. and Y. Lin, 2008. Tumor necrosis factor and cancer, buddies or foes? Acta Pharmacologica Sinica, 29: 1275-1288.
- Picchi, A., X. Gao, S. Belmadani, B.J. Potter, M. Focardi, W.M. Chilian and C. Zhang, 2006. Tumor necrosis factor-α induces endothelial dysfunction in the prediabetic metabolic syndrome. Circ. Res., 99: 69-77.
- Drożdż, D., M. Drożdż and M. Wójcik, 2023. Endothelial dysfunction as a factor leading to arterial hypertension. Pediatr. Nephrol., 38: 2973-2985.
- Holbrook, J., S. Lara-Reyna, H. Jarosz-Griffiths and M.F. McDermott, 2019. Tumour necrosis factor signalling in health and disease. F1000Research, 8.
- Bassuk, S.S. and J.E. Manson, 2015. Oral contraceptives and menopausal hormone therapy: Relative and attributable risks of cardiovascular disease, cancer, and other health outcomes. Ann. Epidemiol., 25: 193-200.
- Wentzensen, N. and A.B. de Gonzalez, 2015. The Pill's gestation: From birth control to cancer prevention. Lancet Oncol., 16: 1004-1006.
- Yousuf, S.D., M.A. Ganie, U. Urwat, S.M. Andrabi and M.A. Zargar et al., 2023. Oral contraceptive pill (OCP) treatment alters the gene expression of intercellular adhesion molecule-1 (ICAM-1), tumor necrosis factor-α (TNF-α), monocyte chemoattractant protein-1 (MCP-1) and plasminogen activator inhibitor-1 (PAI-1) in polycystic ovary syndrome (PCOS) women compared to drug-naive PCOS women. BMC Women's Health, 23.
- Kiley, J. and C. Hammond, 2007. Combined oral contraceptives: A comprehensive review. Clin. Obstet. Gynecol., 50: 868-877.
- Yousuf, S.D., F. Rashid, T. Mattoo, C. Shekhar, S. Mudassar, M.A. Zargar and M.A. Ganie, 2017. Does the oral contraceptive pill increase plasma intercellular adhesion molecule-1, monocyte chemoattractant protein-1, and tumor necrosis factor-α levels in women with polycystic ovary syndrome: A pilot study. J. Pediatr. Adolesc. Gynecol., 30: 58-62.
- Odinga, T.B., C.B. Lemii, I.R. Daka, C.U. Gabriel-Brisibe, S.K. Enebeli, I. Austin-Asomeji and F.U. Edward, 2023. Synergistic mixture of Cyperus esculentus, Phoenix dactylifera and Cocos nucifera aqueous extract: Its liver and kidney benefits in male albino rat model. J. Biosci. Med., 11: 63-75.
- Odinga, T.B., B.C. Lemii, R.I. Daka and S.K. Enebeli, 2022. Assessment on the effect of selected oral contraceptives on the liver functionality and integrity. World J. Biol. Pharm. Health Sci., 9: 46-54.
- Rietzschel, E., M. de Buyzere, D. de Baquer, M. Langlois and S. Bekaert et al., 2007. Oral contraceptives cause major C-reactive protein rises in the female general population. Circulation, 116
- Cauci, S., S. Xodo, C. Buligan, C. Colaninno, M. Barbina, G. Barbina and M.P. Francescato, 2021. Oxidative stress is increased in combined oral contraceptives users and is positively associated with high-sensitivity C-reactive protein. Molecules, 26.
- Park, H., 2022. Association between oral contraceptive use and the high-sensitivity C-reactive protein level in premenopausal Korean women. Healthcare, 10.
- Lee, J., H. Jeong, J.H. Yoon and H.W. Yim, 2022. Association between past oral contraceptive use and the prevalence of hypertension in postmenopausal women: The fifth (2010-2012) Korea National Health and Nutrition Examination Survey (KNHANES V). BMC Public Health, 22..
- Luan, Y.Y. and Y.M. Yao, 2018. The clinical significance and potential role of C-reactive protein in chronic inflammatory and neurodegenerative diseases. Front. Immunol., 9.
- Divani, A.A., X. Luo, Y.H. Datta, J.D. Flaherty and A. Panoskaltsis-Mortari, 2015. Effect of oral and vaginal hormonal contraceptives on inflammatory blood biomarkers. Mediators Inflammation, 2015.
- Banait, T., A. Wanjari, V. Danade, S. Banait and J. Jain, 2022. Role of high-sensitivity C-reactive protein (Hs-CRP) in non-communicable diseases: A review. Cureus, 14.
- Larsen, B., A. Cox, C. Colbey, M. Drew and H. McGuire et al., 2020. Inflammation and oral contraceptive use in female athletes before the Rio Olympic games. Front. Physiol., 11.
- Eagan, L.E., C.A. Chesney, S.E. Mascone, N. Shenouda and S.M. Ranadive, 2021. Interleukin-6 is higher in naturally menstruating women compared with oral contraceptive pill users during the low-hormone phase. J. Appl. Physiol., 131: 544-552.
- Karkhur, S., M. Hasanreisoglu, E. Vigil, M.S. Halim and M. Hassan et al., 2019. Interleukin-6 inhibition in the management of non-infectious uveitis and beyond. J. Ophthalmic Inflammation Infect., 9.
- McCoy, M.K. and M.G. Tansey, 2008. TNF signaling inhibition in the CNS: Implications for normal brain function and neurodegenerative disease. J. Neuroinflammation., 5.
How to Cite this paper?
APA-7 Style
Lemii,
B.C., Daka,
I.R., Gabriel-Brisibe,
C.U., Enebeli,
S.K., Edward,
U.F., Austin-Asomeji,
I., Oghenetekevwe,
E., Chivusalem,
N.C., Odinga-Israel,
T. (2024). Association of Oral Contraceptives Consumption with C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin (IL-6) in Female in vivo Model. International Journal of Biological Chemistry, 18(1), 1-10. https://doi.org/10.3923/ijbc.2024.01.10
ACS Style
Lemii,
B.C.; Daka,
I.R.; Gabriel-Brisibe,
C.U.; Enebeli,
S.K.; Edward,
U.F.; Austin-Asomeji,
I.; Oghenetekevwe,
E.; Chivusalem,
N.C.; Odinga-Israel,
T. Association of Oral Contraceptives Consumption with C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin (IL-6) in Female in vivo Model. Int. J. Biol. Chem 2024, 18, 1-10. https://doi.org/10.3923/ijbc.2024.01.10
AMA Style
Lemii
BC, Daka
IR, Gabriel-Brisibe
CU, Enebeli
SK, Edward
UF, Austin-Asomeji
I, Oghenetekevwe
E, Chivusalem
NC, Odinga-Israel
T. Association of Oral Contraceptives Consumption with C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin (IL-6) in Female in vivo Model. International Journal of Biological Chemistry. 2024; 18(1): 1-10. https://doi.org/10.3923/ijbc.2024.01.10
Chicago/Turabian Style
Lemii, Barizoge, Cletus, Iyaeneomi Ransome Daka, Christine Umanu Gabriel-Brisibe, Sarah Kelechi Enebeli, Ucheawaji Felicia Edward, Iyingiala Austin-Asomeji, Efekemo Oghenetekevwe, Nodi Conquest Chivusalem, and Tamuno-Boma Odinga-Israel.
2024. "Association of Oral Contraceptives Consumption with C-Reactive Protein (CRP), Tumor Necrosis Factor-α (TNF-α) and Interleukin (IL-6) in Female in vivo Model" International Journal of Biological Chemistry 18, no. 1: 1-10. https://doi.org/10.3923/ijbc.2024.01.10

This work is licensed under a Creative Commons Attribution 4.0 International License.